Dilantin® (Phenytoin)
Another AntiConvulsant that is useful for relieving Pain associated with irritating Sensory Loss. It is less effective than Tegretol and also less toxic, but blood tests should also be obtained prior to therapy.
A total dose of 300 mg is the goal, or until partial pain relief is obtained, and then carefully titrate the dose upward. Blood levels should be obtained pre-treatment, and Side-Effect are similar to Tegretol.
Elavil® (Amitriptyline)
Or its milder *cousin* Nortriptyline, and other Tri-Cyclic AntiDepressants are useful in the treatment of Involuntary Facial Movements, Painful Pins & Needles Feelings, and Emotional Outbursts.
Side-Effects: include Dryness of the Mouth, Constipation, and Bladder Hesitancy.
Naprosyn
A Non-Steroidal Anti-Inflammatory, like Motrin and Clinoral, that are useful in reducing Pain and Inflammation. Continuous use at high doses could lead to Gastrointestinal Tract Ulceration and Bleeding.
Neurontin® (Gabapentin)
A new AntiConvulsant that has shown some promise in the treatment of Neuropathic pain. It may be the next reasonable step for those patients not adequately treated with Tegretol or Dilantin.
The drug is increased in 300 mg increments over two days as side-effects allow, until a total dose of 1800 mg daily is reached. Daily dose should not exceed 2400 mg.
Side-Effects: Sedation, Dizziness, & Confusion.
Tegretol® (Carbamazepine)
An AntiConvulsant that relieves pain arising in the Nervous System. Especially helpful in Tic Douloureux.
Start with a 100-200 mg dose of Tegretol at bedtime for two nights and caution the patient regarding Side Effects, including Dizziness, Sedation, Confusion, and Rash.
The drug is in equally divided doses over two days, as Side-Effects allow, until pain relief is obtained or a total dose of 1200 mg daily is reached.
Careful monitoring of lab parameters is mandatory to avoid the rare possibility of life-threatening Blood Dyscrasia. At the first sign of blood count abnormality or rash, Tegretol should be discontinued.
Failure to monitor patients started on Tegretol can be disastrous, as Aplastic Anemia can occur. When pain relief is obtained, the patient should be kept at that dosage at least six months before tapering. Routine Hematologic monitoring after stable dosage is reached is unnecessary.
Tegretol blood levels should be obtained when non-compliance is suspected, when Side-Effect occur at doses under 1200 mg, and when a 1200 mg/day dose is reached, to establish a baseline to allow safe titration of the dosage upward.
Side-Effect: Rashes, Weakness, Drowsiness, & Aplastic Anemia. Low blood cell counts are a rare but possible Side-Effect.
Clonidine®
(Catapres-TTS)
Stimulates  2-AdrenoReceptors in the BrainStem, resulting in reduced Sympathetic outflow from the Central Nervous System and a decrease in peripheral Blood Vessel Resistance, Renal Vascular Resistance, Heart Rate, and Blood Pressure - it is an AntiHypertensive agent. Some find Clonidine is helpful for Spasticity. 2-AdrenoReceptors in the BrainStem, resulting in reduced Sympathetic outflow from the Central Nervous System and a decrease in peripheral Blood Vessel Resistance, Renal Vascular Resistance, Heart Rate, and Blood Pressure - it is an AntiHypertensive agent. Some find Clonidine is helpful for Spasticity.
Common Side-Effects: are Low Blood Pressure 45%, Dizziness 13%, Anxiety 11%, and Dry Mouth 13%.
Dantrium® (Dantrolene)
Is recommended only for Spasticity that does not respond to Lioresal (Baclofen). Brief withdrawal for a period of 2-4 days will result in exacerbations of Spasticity. Long term therapy must meet specific criteria.
Dantrolene is a Muscle Relaxant for relief of the Cramping, Spasms and Tightness of Muscles caused by Multiple Sclerosis. It acts directly on the Muscles.
Side-Effects may include Liver toxicity especially among people who use more than 100 mg per day. Dantrium therapy may cause several Liver Disorders (Fatal and Non-Fatal).
Adverse-Reactions commonly include: Drowsiness, Dizziness, Weakness, General Malaise, Fatigue and an Increase in Photosensitivity.
Lioresal® (Baclofen)
Is given to treat stiffness or Spasticity, the second most common symptom of MS. It can often improve and relive painful Sensory disturbances.
Careful monitoring of lab values is indicated during the initial use of the drug. In treating patients with any of these drugs, the premature tapering or discontinuation of the medication may lead to the recurrence of pain and it will be more difficult to control pain thereafter.
Baclofen has significant Hepatic and Central Nervous System Side-Effects: Increasing Muscle Weakness, Sedation, and Confusion are most common; for these reasons.
It is poorly tolerated by many people and dosages must be slowly lowered before discontinuing its use, since suddenly stopping it, may induce Hallucinations and Seizures.
Valium® (Diazepam)
Is a Benzodiazepine derivative classified as an AntiAnxiety drug that can also be used to help relieve Spasticity. Diazepam appears to act on parts of the Limbic System: the Thalamus & HypoThalamus, inducing a calming effect.
Side-Effects: Drowsiness, Fatigue, and Ataxia. Valium may be addictive.
Zanaflex® (Tizanidine)
Is an 2-Adrenergic Agonist (like Clonidine), it is a short-acting drug for management of Spasticity's increased muscle tone. The reduction of muscle tone has its peak effect 1 to 2 hours, and the benefit dissipates in 3 to 6 hours.
Side-Effects: Tizanidine can produce Hypotension (Low-Blood Pressure), Bradycardia, Light-Headedness/Dizziness and rarely, Syncope.
Common Side-Effects: Sedation, Dry Mouth (49%), Somnolence (48%), Asthenia [Weakness, Fatigue and/or Tiredness (41%)], and Dizziness (16%).
UnCommon Side-Effects: Tizanidine may causes Liver Injury, Nausea, Vomiting, Anorexia, Jaundice, Hallucinosis, and Delusions.
Tremors
Klonopin® (Clonazepam)
Exhibits several pharmacologic properties which are characteristic of the Benzodiazepine class of drugs. Clonazepam can provide some relief from Tremors. It is Very Sedating, producing CNS Depression, so it is useful in just small numbers of patients.
Antivert® (Meclizine)
Helps manage Nausea, Vomiting and Dizziness associated with Motion Sickness and is used in the management of Vertigo that some experience in MS.
Side-Effects include Drowsiness, Dryness of the Mouth, and rarely Blurred Vision.
Diminhydrinate
Is a similar drug related to Benedryl® (Diphenhydramine) that is also used; it inhibits Acetylcholine one of the best known NeuroTransmitters in the Brain.
Transderm Scop® (Scopolamine)
Is an AntiCholinergic drug that helps treat Dizziness, it is a skin patch that lasts for several days.
Potential Adverse-Effects: Confusion, Memory Disturbances, Drowsiness, and Dryness of the Mouth.
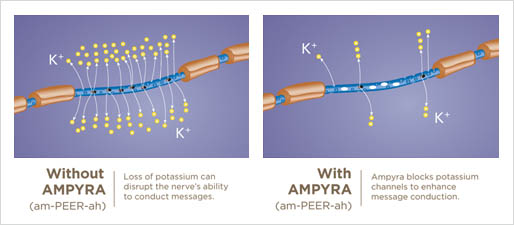
Amypra® (Dalfampridine)
Extended Release Tablets is indicated as a treatment to improve walking in patients with Multiple Sclerosis (MS). This was demonstrated by an increase in walking speed. Amypra is a tablet, taken twice a day about 12 hours apart.
Ampyra is a broad-spectrum Potassium Channel Blocker, and the first MS medication to enhance Impulse Conduction in the nerve fibers whose insulating Myelin layer has been damaged, by blocking some of the Potassium Ion Channels.
Ampyra is thought to block Potassium (K+) Channels. This can make a difference for some people with MS. Ampyra does not replace Potassium, nor is it a Potassium supplement.
It is not known if Ampyra is safe and effective in children less than 18 years of age.
Side-Effects
Do not take Ampyra if you: have ever had a Seizure, it may cause serious side effects, including Kidney or Bladder infections. Your chance of having a Seizure is higher if you take too much Ampyra or if you have Kidney problems.
The most common side effects of Ampyra include: Urinary Tract Infection; trouble Sleeping (Insomnia); Dizziness; Headache; Nausea; Weakness; Back Pain; problems with balance; Multiple Sclerosis relapse; burning, tingling or itching of your skin; irritation in your nose and throat; constipation; indigestion; pain in your throat.
|