Merck Manual
1992 - 16th Edition
#12-00
(Albany Public Library
Reference Desk)
ch 127
p1488
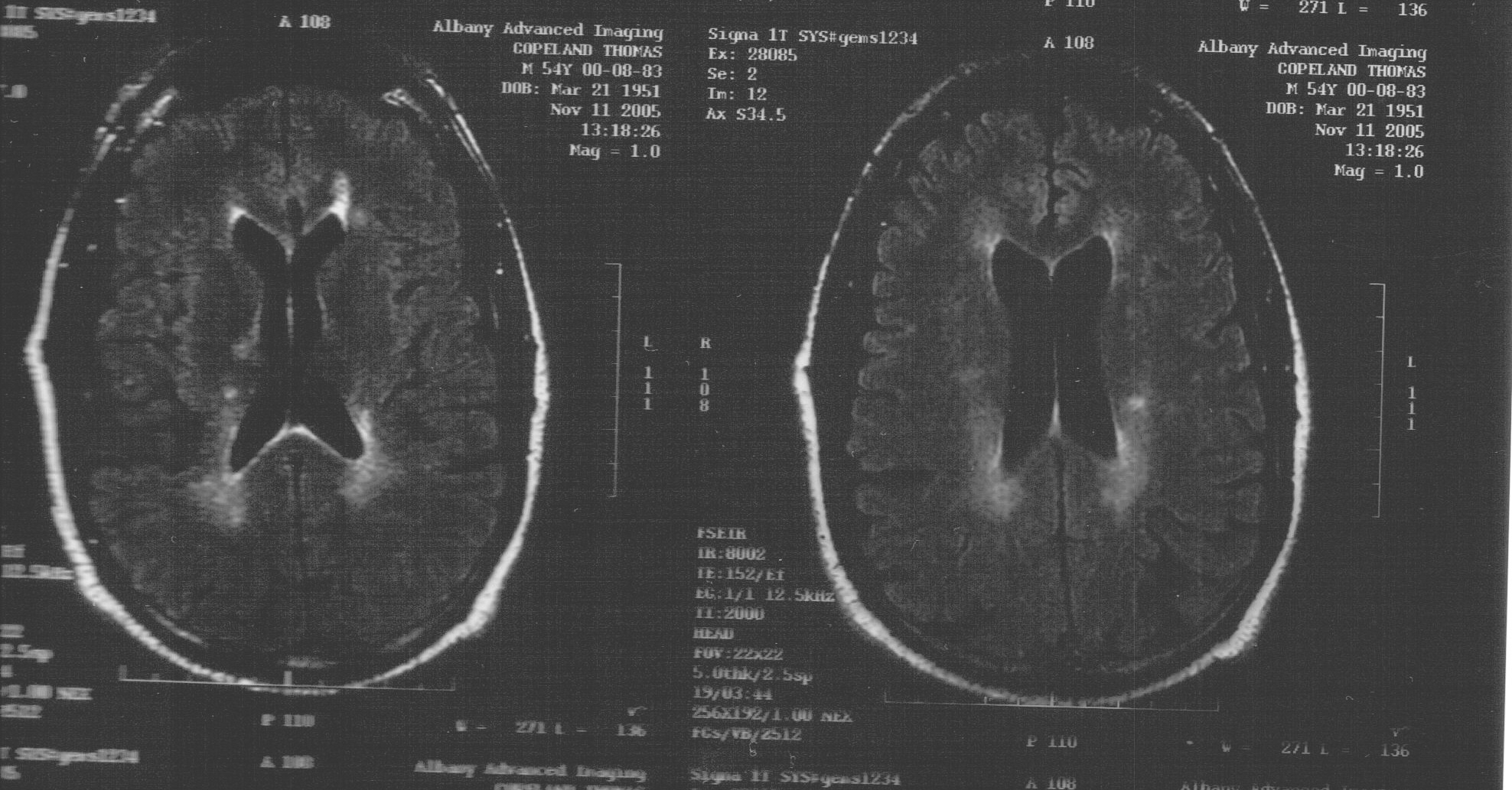
Plaques or islands of DeMyelination with destruction of both Oligodendroglia and PeriVascular Inflammation are disseminated through the CNS, primarily in the White Matter, with a predilection for the Lateral and Posterior Column (esp. in the Cervical and Dorsal regions) the Optic Nerves and PeriVentricular Areas.
Tracts of the MidBrain, Pons and Cerebellum also are affected, and Gray Matter in both Cerebrum and Cord may be affected, Cell bodies and Axons usually are preserved, especially in early Lesions.
Later, Axons may be destroyed, usually in the Long Tracts, and Fibrous Gliosis gives the Tracts their "sclerotic appearance". Both early and late Lesions may be found simultaneously. Chemical changes in Lipid and Protein constituents of Myelin have been demonstrated in and around the Plaques.
Mental
p1489
Apathy, lack of judgment, or inattention may occur. Emotional Lability is common and with widespread mild signs can lead to the incorrect impression of *Hysteria*.
Euphoria occurs in many patients, but in others a reactive Depression is present. Sudden weeping or laughter indicates that CorticoBulbar Pathways of Emotional Control are involved.
Charcot's Triad
(Nystagmus, Intention Tremor, & Scanning Speech) is a common Cerebellar manifestation in advanced disease. Mild Dysarthria may result from Cerebellar damage, disturbance of Cortical Control, or injury to the Bulbar Nuclei.
Course
The course is highly varied and unpredictable and in most patients, remittent. At first, months or years of remission may separate episodes, especially when the disease begins with Retrobulbar Neuritis, but usually the intervals of freedom grow shorter, and eventually permanent, progressive disability occurs.
Remissions have lasted > 25 years. However, some patients have frequent attacks and are rapidly incapacitated; in a few, particularly when onset is in middle age, the course is progressively and unRemittingly downhill, and occasionally fatal within a year.
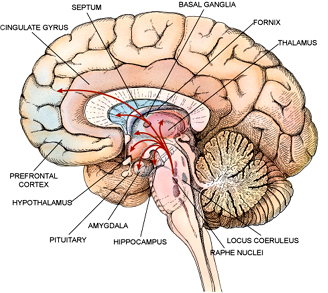
Three Major Components of the Motor System
- The CorticoSpinal (Pyramidal Tracts)
Pass through the Medullary Pyramids to connect the Cerebral Cortex to the lower Motor Centers of the BrainStem and Spinal Cord.
- The Basal Ganglia (Caudate Nucleus, Putamen, Globus Pallidus and Substantia Nigra)
This ExtraPyramidal System, consisting of a group of interrelated structures lying deep in the ForeBrain, whose output is directed mainly rostrally through the Thalamus to the Cerebral Cortex, rather than passing caudally directly through the Pyramidal Tract.
(View Interior Image & Larger Image)
- The Cerebellum
The center for motor coordination that lies on the dorsal surface of the BrainStem. The contributions of these Motor System components towards producing movement are shown by the abnormal movement patterns that remain when a component is damaged or diseased.
Cerebellum's Three Anatomically Subdivisions
ch128
p1500
- The Archi or VestibuloCerebellum: comprises the Flocculonodular Lobe, which is concerned with the maintenance of equilibrium and Eye-Head-Neck movements and is closely interconnected with the Vestibular Nuclei.
The Midline Vermis or PaleoCerebellum: helps coordinate movement of the Trunk and Legs. Vermis lesions result in abnormalities of Stance and Gait.
The Lateral Hemispheres: which make up the NeoCerebellum, exert control over both Ballistic and Finely Coordinated Limb Movements, predominantly of the Upper Extremities.
|
{kind=link}
{kind=link}
{kind=link}